How many parents suffer quietly with the plight of their child’s condition, or keep to themselves for the sake of privacy, or simply are heads down with caregiving that others don’t even know to reach out? I also imagine parents in communities who don’t have the privilege of a well-resourced school system or medical access or aren’t able to rally funds for research or costs of care. The bottom line is that more needs to be done for families to foster the kind of resilience that may be needed for a long haul. Two colleagues (Lorraine Hobbs and Kimberly Arthur) and I recently published a journal article about the need to support parents with children with chronic conditions: The Role of Compassion and Mindfulness in Building Parental Resilience When Caring for Children With Chronic Conditions: A Conceptual Model. (Please read and share it. E-Book here.)
…both mindfulness and compassion have significant potential to support this process of working through adversity and finding ways to develop inner resources to cultivate acceptance, find meaning in the context of complex parenting challenges, and respond to the child and oneself with kindness in the face of persistent stressors associated with children’s chronic conditions.
Cousineau, Hobbs & Arthur, 2019
A Silent Suffering
Parenting a child with an illness or disability is very common yet remains a silent plight for many.
Close to 20% of parents have a child with a chronic condition or disability, which is defined as any condition that has lasted or is expected to last for at least 12 months. Personally, I think this is an underestimate due to under reporting and stigma. But let’s just say that 1 in 5 parents/families has a child with some sort of chronic affliction. (There are 83M families in the US and 15M single mothers.) Assume for the sake of my argument that you are in a room full of parents. The next time you are in a meeting at work or a school PTA meeting, or at a place of worship, or on a commuter train imagine that for every 4 seats the 5th seat has a parent facing a difficult illness challenge with a child—no matter the age of a child. Imagine yourself in his or her shoes.
The school eventually became “peanut/nut free” to the chagrin of other parents. It was a common battle cry across American schools: “Why should my child give up his PB&J?” “That’s the only thing he eats and he has the right to have peanut butter.” “Why should my kid starve?” Parents of the afflicted child would counter, “This could be a life or death situation. Surely you can see that?” “You’d rather see a child risk her life than to find something else for your kid to eat?” “Try carrots instead.”
Later the solution in the elementary school was to separate the food allergy kids from the others at lunch time, leaving Sophie at a table all by herself. She became a pariah, a social outcast. The social stigma was an unintended consequence, of course. And it was unacceptable.
Then guess what happened? God bless the children to find solutions that parents or administrators can’t see. Her friends began to sit with her. Over time they became little vigilantes monitoring who had what in their lunch boxes. The girls made sure their parents knew about Sophie’s food allergies for birthday parties and sports events. They educated themselves. They watched the Epi-pen injection video and practiced puncturing an orange with a plastic model pen. Although we were all in a state of anticipatory anxiety, organically we cultivated a “community watch.” Eventually, we all relaxed. When a local 15-year old girl died from anaphylaxis after a severe allergic reaction just days before her 16th birthday, despite the family’s careful precautions, the threat became all too real once again. (See Project Abbie at Harvard.)
Compassionate Action
My daughter’s situation may not compare to the plight of others. A food allergy is an episodic condition that is largely reliant on prevention and avoidance, yet can have a fatal outcome. Yet that’s not my point. Millions of parents are managing some sort of childhood condition every single day. Of course, the medical conditions and potential outcomes vary among children: Children may be hospitalized for depression or suicidal ideation, or suffer a physical illness or condition; or a child may be contending with developmental delays, mobility issues, aggressive outbursts, or chronic pain. There are IEPs and accommodations, specialists, and regular medical monitoring, and concerns about independent living in adulthood. It can be all consuming at times.
What is common is the persistent fear and distress felt by a mom, dad or caregiver. Whenever a child needs specialized care or attention, there is a slow wear-and-tear in the fabric of parenting. An unraveling may occur in parallel with a kind of constant mending, in attempts to emotionally or pragmatically hold it together. There is also the mental “code switching” between taking care of a child’s current needs and the anticipation or planning for the future “what ifs.” It’s hard to be present when the mind is in a ricochet of tending tasks. Let’s not forget that many parents inevitably put their personal needs and goals on hold and may also be economically impacted. Even the most optimistic or well-resourced parents will find themselves in moments of despair or panic. That’s the only natural response.
The emotions that drive defensive behavior include anger, anxiety, fear, or disgust. When we notice which emotion regulation systems are activated (threat, thrive, care/connect), we can begin to respond to life’s experiences in more beneficial and grounded ways. We can respond in a more balanced way. This is where mindfulness and compassion comes in.
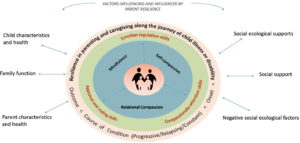
Cousineau, Hobbs, and Arthur. The Role of Compassion and Mindfulness in Building Parental Resilience When Caring for Children With Chronic Conditions: A Conceptual Model
The approach we proposed in the article emphasizes relational compassion and self-compassion. All too often the sole or primary focus is on child medical outcomes rather than parental resilience. This is understandable but to use another cliché—the one about the oxygen mask on a flight—we have to help the caregivers put on the oxygen mask first. The point in our article is we believe that cultivation of safety, connection, and caring is essential in any communication, intervention, or resource created to support parents when caring for a child with a chronic condition. This helps to get parents out of the constant threat/survival mode and offer relief from the exhaustion that can come from empathy fatigue, persistent uncertainty, constant caregiving, or social isolation. This means growing both inner strengths and outer strengths.
We consider the mindfulness and compassion skills as a way to “bounce forward” rather than “bounce back”—because life will never revert to a previous way of parenting. Resilience is inherently about caring, connection and community. It also requires a kind of deep knowing that we all belong to one another. In this way we are responsible for the welfare of the collective “we.” Parenting is hard under optimal circumstances. No family is immune from threat, loss, or disappointment. It can take some emotional courage to turn toward what is difficult and reach out to a family in helpful ways—especially when vulnerable children face challenges. The default is to respect privacy, or not impose, or keep a safe distance, or drop off casseroles. I get it. But we also have to stretch ourselves and connect with parents. We don’t know what we don’t know.
Take the risk: Ask them.
How may I be of help? Is there something specific I can do? What is important for us to know? Is it Ok if I check in every once in a while? We are here for you.